GENERAL MEDICINE ONLINE ASSIGNMENT
Name: Rishitha Rao.K
Roll.no:180
MBBS 8th sem
I have been given the following cases to solve in an attmept to understand the topic of 'Patient clinical data analysis' to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and diagnosis and come up with a treatment plan.
This is the link of the questions asked regarding the cases:
PULMONOLOGY
CASE 1
1)A 55-year-old female with shortness of breath ,pedal Edema ,and facial puffiness.
https://soumyanadella128eloggm.blogspot.com/2021/05/a-55-year-old-female-with-shortness-of.html
a)the anatomical localization of the problem is at the bronchioles.
etiology-its is due exposue of dust /allergens in paddy feilds
b)PHARMACOLOGICAL INTERVENTION
head end elevation
MECHANISM:In an intervention study involving early mobilization of intubated abdominal surgery patients, it was observed that high thoracic positions, such as sitting upright for 20 minutes, led to an improvement in transthoracic pressure, with consequent improvement in the Cst, rs. This gain enabled a reduction in the driving pressure required for the generation of a similar lung volume.
BiPAP
MECHANISM: During systole, CPAP induced increase in intrathoracic pressure reduces the venous return, decreasing the right and left ventricular preload, thereby improving mechanics in an overloaded ventricle, whereas in diastole, CPAP increases pericardial pressure, reduces transmural pressure, and thus decreases afterload.
Agumentin(amoxicillin+calvulanic acid)
MECHANISM: Amoxicillin binds to penicillin-binding proteins within the bacterial cell wall and inhibits bacterial cell wall synthesis. Clavulanic acid is a β-lactam, structurally related to penicillin, that may inactivate certain β-lactamase enzymes
Azithromycin
MECHANISM: Azithromycin binds to the 23S rRNA of the bacterial 50S ribosomal subunit. It stops bacterial protein synthesis by inhibiting the transpeptidation/translocation step of protein synthesis and by inhibiting the assembly of the 50S ribosomal subunit
inj.lasix
MECHANISM: Furosemide, like other loop diuretics, acts by inhibiting the luminal Na-K-Cl cotransporter in the thick ascending limb of the loop of Henle, by binding to the chloride transport channel, thus causing sodium, chloride, and potassium loss in urine.
tab.Pantop
MECHANISM: The mechanism of action of pantoprazole is to inhibit the final step in gastric acid production. In the gastric parietal cell of the stomach, pantoprazole covalently binds to the H+/K+ ATP pump to inhibit gastric acid and basal acid secretion. The covalent binding prevents acid secretion for up to 24 hours and longer.
inj. hydrocortisone
MECHANISM:Hydrocortisone binds to the glucocorticoid receptor leading to downstream effects such as inhibition of phospholipase A2, NF-kappa B, other inflammatory transcription factors, and the promotion of anti-inflammatory genes. Hydrocortisone has a wide therapeutic index and a moderate duration of action.
Neb. with ipravent ,budecortisone
MECHANISM:
*Ipravent belongs to a group of medicines known as anticholinergic bronchodilators. Anticholinergic bronchodilators work by relaxing the bronchial tubes (air passages) that carry air in and out of your lungs. This makes breathing less difficult.
*Budesonide is a potent topical anti-inflammatory agent. [19] It binds and activates glucocorticoid receptors (GR) in the effector cell (e.g., bronchial) cytoplasm that allows the translocation of this budesonide-GR complex in the bronchi nucleus, which binds to both HDCA2 and CBP
tab.pulmoclear
MECHANISM: Pulmoclear Tablet is a combination of two mucolytic medicines: Acebrophylline and Acetylcysteine. It thins and loosens mucus (phlegm) making it easier to cough out.
chest physiotherapy
MECHANISM:The aims of ACTs in patients with COPD are to assist sputum clearance in an attempt to reduce symptoms and paroxysmal coughing, slow the decline in lung function, reduce exacerbation frequency and hasten the recovery from exacerbations.
inj.thiamine
MECHANISM:thiamine may augment aerobic metabolism in the critically ill, even in the absence of absolute deficiency. We hypothesized that the administration of intravenous thiamine to critically ill patients would cause an increase in oxygen extraction and V.o2.
BP,PR,SPO2,Temp
MECHANISM: All 3 vital signs acquired from a pulse oximeter (pulse rate, oxygen saturation, and respiratory rate) are predictive of COPD exacerbation events, with oxygen saturation being the most predictive, followed by respiratory rate and pulse rate.
I/O charting
MECHANISM: Fluid overload or pulmonary/vascular congestion is a common clinical feature in patients with heart failure and is associated with adverse outcomes. Maintaining records of patients' fluid intake and output (I&O) has long been considered an important aspect of nursing care to assess hydration status.
c) The cause of acute Exaberation in this patient is probably due to generalised weakness due to the drugs or due to upper respiratory tract infection.
d)ATT could have effected the patient’s condition by causing generalised weakness.
e)*Hyponatraemia in COPD develops due to many reasons such as worsening of hypoxia, hypercapnia ,respiratory acidosis and right-sided heart failure with development of lower limb oedema ,it could also be due to renal insufficiency.
NEUROLOGY
1.9 days ago falling and laughing to himself which is of sudden onset
Decreased food intake - 9 days
Short term memory loss since 9 days
One episode of seizures 1 year ago
And another episode if seizure 4 months ago following cessation of alcohol associated with sweating
The problem is with the neurotransmitters
Etiology being alcohol intake
Alcohol is generally known as a DEPRESSANT of the central nervous system; it INHIBITS brain activities, causing a range of physiological effects.
The pleasurable feeling associated with drinking, on the other hand, is linked to alcohol-induced dopamine release
Alcohol also increases levels of brain serotonin, a neurotransmitter implicated in mood regulation.
Short-term alcohol consumption DISRUPTS this balance, INCREASING INHIBITORY and DECREASING EXCITATORY functions.
It triggers GABA receptors, ligand-gated chloride channels, to open and allow chloride ions to flow into the neuron, making it more NEGATIVE and LESS likely to respond to new stimuli (keeping the channels open for a longer time and thus exaggerating this inhibitory effect)
long-term consumption of alcohol, however, produces an OPPOSITE effect on the brain. This is because SUSTAINED inhibition caused by PROLONGED alcohol exposure eventually ACTIVATES the brain's ADAPTATION
In attempts to restore the equilibrium, the brain DECREASES GABA inhibitory and INCREASES glutamate excitatory functions to compensate for the alcohol's effect. As the balance tilts toward EXCITATION, more and more alcohol is needed to achieve the same inhibitory effect. This leads to overdrinking and eventually addiction.
2.IVF NS and RL: Administer intravenous (IV) fluids for rehydration, as necessary. Most patients with severe alcohol withdrawal are significantly dehydrated, and their fluid requirements range from 4-10 L in the first 24 hours. Because hypoglycemia is common in these patients due to depleted glycogen stores, a 5% dextrose solution (in 0.90% or 0.45% saline) should be used to prevent hypoglycemia.
THIAMINE: chronic alcohol consumption can result in thiamine deficiency by causing inadequate nutritional thiamine intake, decreased absorption of thiamine from the gastrointestinal tract, and impaired thiamine utilization in the cells.
Lorazepam : Benzodiazepines are the mainstay of treatment in alcohol withdrawal. Benzodiazepines are cross-tolerant with alcohol and modulate anxiolysis by stimulating GABA-A receptors.During withdrawal from one agent, the other may serve as a substitute. They are proven to reduce withdrawal severity and incidence of both seizures.
Pregabalin:Pregabalin is a structural analogue of GABA approved by FDA for partial epilepsy, neuropathic pain and recently generalized anxiety disorder.
Syp Potchlor:it helps to maintain potassium balance in the body by restoring normal potassium 4.Thiamine is required for carbohydrate metabolism
It acts as a coenzyme.
Thymine pyrophosphate is required in:
Pyruvate dehydrogenase ketoglutarate dehydrogenase.
Branched chain ketoacid dehydrogenase.
Transketolase
Thiamine deficiency may lead to wernikes encephalopathy
In order to prevent it we give thiamine supplements
5. Alcohol induced kidney injury
6.Chronic excessive alcohol ingestion reduces the number of blood cell precursors in the bone marrow and causes characteristic structural abnormalities in these cells, resulting in fewer-than-normal or non functional mature blood cells. As a result, alcoholics may suffer from moderate anemia, characterized by enlarged, structurally abnormal RBC's
Or it may be due to
Hypersplenism, a condition charac terized by an enlarged spleen and can induce premature RBC destruction
7.Drinking high amounts of alcohol may be linked to increased risk of stroke or peripheral artery disease - the narrowing of arteries in the legs
This is thought to preven t adequate blood flow to the tissue in the leg. As a result, this tissue will die, and ulcers will begin to form or fail to heal
52 year old male with cerebellar ataxia.
https://kausalyavarma.blogspot.com/2021/05/a-52-year-old-male-with-cerebellar.html?m=1
- What is the evolution of the symptomatology in this patient in terms of an event timeline and where is the anatomical localization for the problem and what is the primary etiology of this patient?
Evolution of symptomatology
- On 13/5/2021- Giddiness and vomiting
- On 16/5/2021- Giddiness: sudden onset, gradual progression bilateral hearing loss, aural fullness, tinnitus. Vomiting of 2 episodes per day non bilious
- On 18/5/2021- slurring of speech, deviation of mouth
Anatomical localization
- Right inferior cerebellar hemisphere
Primary etiology
Alcohol intake and persistent not properly treated hypertension
- What are the mechanism of action, indication and efficacy over placebo of each of the pharmacological and non pharmacological interventions used for this patient?
Mode of action- Histamine analogue
Indication- Dizziness
Mode of action- Inhibits serotonin by blinding to serotonin receptors
Indication- Nausea and vomitting
Mode of action- antiplatelet action by inhibiting formation of thromboxane A2
Indications- infarct in brain
Mode of action- HMG CoA reductase inhibitor
Indications- High serum cholesterol
Mode of action- inhibits platelet aggregation
Indications- infarct in brain
Mode of action- thiamine supplement
Indications- thiamine deficiency
Mode of action- supplements cobalamin (vitamin B12)
Indications- Vitamin B12 deficiency
- Did the patient’s history of de novo HTN contribute to his current condition?
- Yes, the patient’s condition can be attributed to not only these habits posing as potential risk factors (mainly chronic alcohol intake in this case), but also long standing or persistent HTN for which he wasn’t consistent with treating it using medication.
- This sort of cause leads to haemorrhagic type of stroke that directly damages brain tissue or obstructs vascular flow through local elevated pressure.
- Does the patients history of alcoholism make him more susceptible to ischemic or haemorrhagic type of stroke?
- The patient’s alcoholism makes him more susceptible to haemorrhagic type of stroke also paired with the patient’s HTN being an even bigger risk factor.
- Alcohol is said to decrease the levels of liver produced coagulation factors and brings about platelet abnormalities all of which predispose to haemorrhagic strokes.
NEUROLOGY
https://amishajaiswal03eloggm.blogspot.com/2021/05/a-50-year-old-patient-with-cervical.html
Q) What is myelopathy hand ??
Loss of power of adduction and extension of the ulnar two or three fingers and an inability to grip and rapidly release with these fingers is termed as myelopathy hand. This is due to Pyramidal Tract Involvement.
It is a neurological sign consisting of involuntary abduction of the fifth finger due to unopposed action of the the extensor digiti minimi. This is seen in cervical myelopathy.
Q) What is Hoffmans Reflex ??
It is a test used to examine the reflexes of upper extremities.
It tests for the possible existence of spinal cord compression.
NEUROLOGY
https://rishikoundinya.blogspot.com/2021/05/55years-old-patient-with-seizures.html
Q) Is there any relationship between occurrence of seizure to brain stroke. If yes what is the mechanism behind it?
Seizures after haemorrhagic strokes are thought to be attributable to irritation caused by products of blood metabolism. The exact pathophysiology is unclear, but an associated ischaemic area secondary to haemorrhage is thought to play a part. Late onset seizures are associated with the persistent changes in neuronal excitability and gliotic scarring is most probably the underlying cause.
NEUROLOGY (F)
http://shivanireddymedicalcasediscussion.blogspot.com/2021/05/a-30-yr-old-male-patient-with-weakness.html
Q) 1.Does the patient's history of road traffic accident have any role in his present condition?
A:One cause of stroke after trauma is a tear in the head or neck blood vessels that lead to the brain, which can be a source of blood clots that cause a stroke. If a tear in these arteries can be diagnosed at the time of the trauma, a patient could be treated with an anti-clotting medicine to help prevent stroke
2.What are warning signs of CVA??
- Sudden NUMBNESS or weakness of face, arm, or leg, especially on one side of the body.
- Sudden CONFUSION, trouble speaking or understanding speech.
- Sudden TROUBLE SEEING in one or both eyes.
- Sudden TROUBLE WALKING, dizziness, loss of balance or coordination.
- Sudden SEVERE HEADACHE with no known cause.
3) What is the Drug rationale in CVA??
Aspirin - Anti Platelet
Atorvastatin - Decreases the level of Plasma LDL
Clopidogrel
4. Does alcohol has any role in his attack?
Heavy alcohol consumption has been associated with an increased risk of stroke and stroke mortality. In addition to alcohol consumption, the most important risk factors for stroke are hypertension, coronary artery disease, cardiac insufficiency, atrial fibrillation, type 2 diabetes, smoking, overweight, asymptomatic carotid artery stenosis and elevated levels of cholesterol.
5.Does his lipid profile has any role for his attack??
Yes increased LDL causes atherosclerosis which ultimately results in stroke.
CARDIOLOGY : case 1
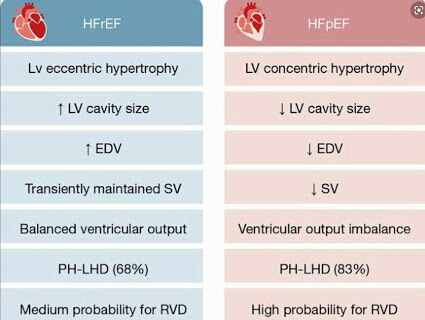
1.What is the difference btw heart failure with preserved ejection fraction and with reduced ejection fraction?
Ans:Preserved ejection fraction (HFpEF) – also referred to as diastolic heart failure. The heart muscle contracts normally but the ventricles do not relax as they should during ventricular filling (or when the ventricles relax).
Reduced ejection fraction (HFrEF) – also referred to as systolic heart failure
HFpEF is preceded by chronic comorbidities, such as hypertension, type 2 diabetes mellitus (T2DM), obesity, and renal insufficiency, whereas HFrEF is often preceded by the acute or chronic loss of cardiomyocytes due to ischemia, a genetic mutation, myocarditis, or valvular disease
2.Why haven't we done pericardiocenetis in this pateint?
Ans: Pericardiocentesis is not done here Because the effusion was self healing ,It reduced from 2.4cm to 1.9 cm.
3.What are the risk factors for development of heart failure in the patient?
Ans: risk factors for development of heart faliure in this patent
Alcohol abuse increases the risk of atrial fibrillation, heart attack and congestive heart failure
high blood pressure
Smoking
Diabetes
AV block can be associated with severe bradycardia and hemodynamic instability. It has a greater risk of progressing to third-degree (complete) heart block or asystole.
wosening of pericardial effusion leaing to cardiac tamponade.
4.What could be the cause for hypotension in this
Ans : visceral pericardium may have thickened which is restricting the heart to expand causing hypotension
(May be secondary to TB)
CARDIOLOGY : case 2
QUESTION: What are the possible causes for heart failure in this patient?
The patient has various comorbidities which could have led to a heart failure
1. The patient was diagnosed with type 2 diabetes mellitus 30 years ago and has been taking human mixtrad insulin daily and was also diagnosed with diabetic triopathy indicating uncontrolled diabetes which is major risk factor for heart failure
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5494155/
2. The patient was also diagnosed with hypertension 19 yrs. ago which is also a risk factor for heart failure
https://pubmed.ncbi.nlm.nih.gov/31472888/
3. He is a chronic alcoholic since 40 years which is a risk factor towards heart failure
https://www.nmcd-journal.com/article/S0939-4753(19)30360-6/fulltext
The findings in this article provide longitudinal evidence that moderate and heavy alcohol consumption are associated with decreased LVEF and trend towards a higher risk of incident LV systolic dysfunction, compared to light drinkers.
4. The patient has elevated creatinine and AST/ALT ratios is >2 and was diagnosed with chronic kidney disease stage IV. CKD is also one of the risk factors for heart failure
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2900793/
QUESTION: what is the reason for anaemia in this case?
The patient has normocytic normochromic anaemia. it could be anaemia of a chronic disease as the patient is diagnosed with CKD stage IV.
Chronic kidney disease results in decreased production of erythropoietin which in turn decreases the production of red blood cells from the bone marrow.
Patient’s with anaemia and CKD also tend to have deficiency in nutrients like iron, vitamin B12 and folic acid essential in making healthy red blood cells
QUESTION: What is the reason for blebs and non-healing ulcer in the legs of this patient?
The most common cause for blebs and non-healing ulcer in this patient is diabetes mellitus. CKD is also known to cause delay in healing of wounds along with poorly controlled diabetes. Anaemia can also slow down the process of healing due to low oxygen levels.
QUESTION: What sequence of stages of diabetes has been noted in this patient?
There are 4 stages in type 2 diabetes- insulin resistance, prediabetes, type 2 diabetes and type 2 diabetes and vascular complications, including retinopathy, nephropathy or neuropathy and, or, related microvascular events.
The patient is diagnosed with diabetic triopathy exhibiting sequence of neuropathy, retinopathy and nephropathy
The patient has been diagnosed with diabetic retinopathy, CKD stage IV and shows signs of diabetic neuropathy such as numbness
CARDIOLOGY :case 3
1) What is the evolution of the symptomatology in this patient in terms of an event timeline and where is the anatomical localization for the problem and what is the primary etiology of the patient's problem?
Ans: *the anatomical site is BLOOD VESSELS;
* ETIOLOGY:
The physical stress of hypertension on the arterial wall also results in the aggravation and acceleration of atherosclerosis, particularly of the coronary and cerebral vessels. Moreover, hypertension appears to increase the susceptibility of the small and large arteries to atherosclerosis.
The most likely cause of arterial thrombosis is artery damage due to atherosclerosis. Atherosclerosis occurs when a person has a buildup of plaque on the walls of their arteries. The arteries then begin to narrow and harden, which increases a person's risk of developing arterial thrombosis.
2) What are mechanism of action, indication and efficacy over placebo of each of the pharmacological and non pharmacological interventions used for this patient?
Ans: PHARMACOLOGICAL INTERVENTIONS
1. TAB. Dytor
mechanism: Through its action in antagonizing the effect of aldosterone, spironolactone inhibits the exchange of sodium for potassium in the distal renal tubule and helps to prevent potassium loss.
2. TAB. Acitrom
mechanism: Acenocoumarol inhibits the action of an enzyme Vitamin K-epoxide reductase which is required for regeneration and maintaining levels of vitamin K required for blood clotting
3. TAB. Cardivas
mechanism:Carvedilol works by blocking the action of certain natural substances in your body, such as epinephrine, on the heart and blood vessels. This effect lowers your heart rate, blood pressure, and strain on your heart. Carvedilol belongs to a class of drugs known as alpha and beta-blockers.
4. INJ. HAI S/C
MECHANISM:Regulates glucose metabolism
Insulin and its analogues lower blood glucose by stimulating peripheral glucose uptake, especially by skeletal muscle and fat, and by inhibiting hepatic glucose production; insulin inhibits lipolysis and proteolysis and enhances protein synthesis; targets include skeletal muscle, liver, and adipose tissue
5.TAB. Digoxin
mechanism:
Digoxin has two principal mechanisms of action which are selectively employed depending on the indication:
Positive Ionotropic: It increases the force of contraction of the heart by reversibly inhibiting the activity of the myocardial Na-K ATPase pump,
an enzyme that controls the movement of ions into the heart.
6. Hypoglycemia symptoms explained
7. Watch for any bleeding manifestations like Petechiae, Bleeding gums.
8. APTT and INR are ordered on a regular basis when a person is taking the anticoagulant drug warfarin to make sure that the drug is producing the desired effect.
3) What is the pathogenesis of renal involvement due to heart failure (cardio renal syndrome)? Which type of cardio renal syndrome is this patient?
Ans: *cardiorenal syndrome type 4 is seen in this patient.
4) What are the risk factors for atherosclerosis in this patient?
Ans: effect of hypertention
They can also impair blood vessels' ability to relax and may stimulate the growth of smooth muscle cells inside arteries. All these changes can contribute to the artery-clogging process known as atherosclerosis.
5) Why was the patient asked to get those APTT, INR tests for review?
Ans: APTT and INR are ordered on a regular basis when a person is taking the anticoagulant drug warfarin to make sure that the drug is producing the desired effect.
Here, an INR of 3-4.5 is recommended. Warfarin should be started in conjunction with heparin or low molecular weight heparin when the diagnosis of venous thromboembolism is confirmed, although local protocols may vary in their starting doses and titration schedule.
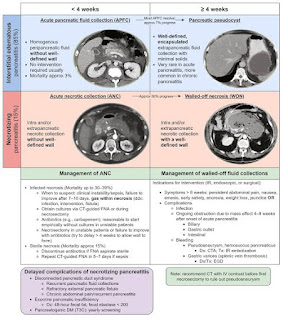
1) What is the evolution of the symptomatology in this patient in terms of an event timeline and where is the anatomical localization for the problem and what is the primary etiology of the patient's problem?
Ans: Patient was apparently asymptomatic 5 yrs back when he had pain abdomen & vomiting. He was symptom free for nearly 3 yrs. Last binge of alcohol was 1 week back following which he again had pain abdomen & vomiting from 1 week and fever from 4 days. Then he developed constipation since 4 days and passing flatus. patient also had burning micturition since 4 days. The problem can be localised to pancreas. The cause of pancreatitis here may be attributed to alcohol.
2) What is the efficacy of drugs used along with other non pharmacological treatment modalities and how would you approach this patient as a treating physician?
Ans: 1) ING. MEROPENAM ; TID for 7 days
* Meropenem ( broad spectrum Carbepenem ) an antibiotic.
2) ING. METROGYL 500 mg IV TID for 5 days
* inj. Metrogyl has METRONIDAZOLE
( Nitroimidazole drug ) an antibiotic
3) ING. AMIKACIN 500 mg IV BD for 5days
* It is an Aminoglycoside antibiotic
## Here all three of these (Inj. Meropenem, Inj. Metrogyl, Inj. Amikacin ) are used as antibiotics to control infection and ; to prevent septic complications of acute pancreatitis.
4) TPN ( Total Parenteral Nutrition )
* Method of feeding that by passes gastrointestinal tract
* Fluids are given to vein , it provides most of the nutrients body needs.
* TPN has proteins, carbohydrates, fats, vitamins, minerals.
5) IV NS / RL at the rate 12l ml per hour
* Given for fluid replacement ie., treat dehydration
6) ING. OCTREOTIDE 100 mg SC , BD
* It is a Somatostatin long acting analogue.
* It is used here to decrease exocrine secretion of pancreas and it also has anti- inflammatory & cytoprotective effects.
7) ING. PANTOP 40 mg IV , OD
* Inj. Pantop has PANTOPRAZOLE ( Proton Pump Inhibitor) used for its anti pancreatic secretory effect.
8) ING. THIAMINE 100 mg in 100 ml NS IV , TID
* It is B1 supplement.
* It is given here because; due to long fasting & TPN usage , body may develop B1 deficiency
* Wernicke encephalopathy secondary to B1 deficiency may be caused... so a prophylactic B1 supplemention is necessary.
9) ING. TRAMADOL in 100 ml NS IV , OD
* It is an opioid analgesic, given to relieve pain.
B)1) what is the most probable diagnosis in this patient?
Ans: Intra peritoneal haemorrhage.
2) What was the cause of her death?
Ans: Haemorrhage is the loss of blood components from the cardiovascular system. Hemorrhagic shock occurs when this blood loss leads to inadequate tissue oxygenation. This could've caused her death.
3) Does her NSAID abuse have something to do with her condition? How?
Ans: Non steroidal anti-inflammatory drugs (NSAIDs) are effective anti-inflammatory and analgesic agents and are among the most commonly used classes of medications worldwide. However, their use has been associated with potentially serious dose-dependent gastrointestinal (GI) complications such as upper GI bleeding. This could've caused haemorrhage in her.
SECTION 5: (NEPHROLOGY)
A)
1. What could be the reason for his SOB ?
Ans: Acute kidney failure may lead to a buildup of fluid in your lungs, which can cause shortness of breath.
2. Why does he have intermittent episodes of drowsiness ?
Ans: High levels of potassium in the blood – in severe cases, this can lead to muscle weakness, paralysis and heart rhythm problems. fluid in the lungs (pulmonary oedema) acidic blood (metabolic acidosis) – which can cause nausea, vomiting, drowsiness and breathlessness.
3. Why did he complaint of fleshy mass like passage in his urine?
Ans: It is probably due to the associated kidney infection.
4. What are the complications of TURP that he may have had?
Ans:
bleeding during the surgery, which requires a transfusion,
improper fluid absorption,
salt imbalances caused by fluid absorption issues,
Impotence (erectile dysfunction),
Incontinence,
urethral stricture (narrowing) leading to a “split stream” of urine,
post-TURP syndrome.
B)
1.Why is the child excessively hyperactive without much of social etiquettes ?
Ans: Attention deficit hyperactivity disorder (ADHD) is a mental health disorder that can cause above-normal levels of hyperactive and impulsive behaviours. People with ADHD may also have trouble focusing their attention on a single task or sitting still for long periods of time. Both adults and children can have ADHD.
2. Why doesn't the child have the excessive urge of urination at night time ?
Ans: Overactive bladder (OAB) represents a syndrome characterised by a myriad of lower urinary tract symptoms (LUTS) including urinary urgency, with or without urgency incontinence, usually with frequency and nocturia, in the absence of infection or other identifiable causes. The true nature of OAB remains elusive – myogenic changes, neurologic changes, urothelial changes and afferent sensitization have been hypothesized to contribute to the symptomatology of OAB. Here it the urge of urination could be psychosomatic due to which at night time he doesn't have it.
3. How would you want to manage the patient to relieve him of his symptoms?
Ans: Principles of treatment are to reduce urinary incontinence by changing patient behaviour and teaching continence skills. As OBS is a symptom complex, 'no treatment' is an acceptable choice for some patients and
6) INFECTIOUS DISEASE
A) https://vyshnavikonakalla.blogspot.com/2021/05/a-40-year-old-lady-with-dysphagia-fever.html
Q) 1.Which clinical history and physical findings are characteristic of tracheo esophageal fistula?
Laryngeal Crepitus,Difficulty in swallowing initially to the solids,
Cough,are Suggestive of TracheoEsophageal Fistula.
Q) What are the chances of this patient developing immune reconstitution inflammatory syndrome? Can we prevent it?
Risk Factors For Development of Immune Reconstitution Inflammatory Syndrome (IRIS)
1) Low Baseline CD4 Count
2) Higher Baseline Viral Load
3) Shorter Interval between commencing ATT and HAART
4) Disseminated TB
5) A Greater Decrease in Viral Load after starting HAART.
As this patient has a low baseline CD4 count and also disseminated TB there are chances that this patient may develop
If the following symptoms are seen after the Initiation of ART then IRIS can be suspected
1) Fever,Anemia,Wt loss.
2) CNS
3) Lymphadenopathy
4) Radiological Findings
5) Exacerbation of Pulm. Lesion or occurence Of a new Lesion.
Prevention of IRIS :
CD4+ T cell deficiency when ART is commenced is a risk factor for an IRIS, prevention of CD4+ T cell depletion through early diagnosis and treatment of HIV infection regardless of CD4+ T cell count, as supported by the findings of the START study (33), is the most effective measure for reducing the risk of developing an IRIS.
However, 'late presenters' with advanced immunodeficiency continue to present and they must be assessed carefully for HIV-related infections that might trigger an IRIS when ART is commenced.
7th Question (B)
https://63konakanchihyndavi.blogspot.com/2021/05/case-discussion-on-liver-abcess.html
1) Cause of liver Abcess in this Patient??
May be due to malnutrition and lack of personal hygeine is the cause of the infection in the patient resulting in liver abcess. The infection may be amoebic or any other bacterial infection.
2) How do you approach this Patient??
As the patient presented with the pain in the abdomen, first I would go for a USG abdomen and As USG showing hyperechoic mass on the liver I would also do LFT(Liverfunction Test)
As there is a mass as seen in USG and LFT is also abnormal (Raised ALP), I would start empirical Treatment for both Amoebic and pyogenic liver abscess.
According to the response given to this Medical Treatment it will be decided whether aspiration is required or not.
3) why do we treat both amoebic and pyogenic liver abscess ??
Even though amoebic liver abscess is confirmed as a diagnosis there is a chance of super infection with bacterial organisms so there is a need for treating both amoebic liver abscess and pyogenic liver abscess
4) Is there a way to confirm definitely diagnosis in this patient ??
Amoebic liver abscess can be confirmed by serology for entamoeba.
7 (A) Infectious Disease and Hepatology
https://kavyasamudrala.blogspot.com/2021/05/liver-abscess.html
Liver abscess
1Q) Do you think drinking locally made alcohol caused liver abscess in this patient due to predisposing factors present in it ??
Yes, may be the liver Abcess developed due to the chronic intake of contminated Toddy.
2) What is the etiopathogenesis of liver abscess in a chronic alcoholic patient ? ( since 30 years - 1 bottle per day)
Chronic alcohol intake especially the locally available contaminated drinks plays a major role in the formation of liver abscesses which can be either Amoebic or Pyogenic liver abscess because of the adverse effects of alcohol over the Liver.
3) Is Liver Abcess more common in Right Lobe ??
50% of solitary liver abscesses occur in the right lobe of the liver (a more significant part with more blood supply), less commonly in the left liver lobe or caudate lobe.
4) what are the indications of Ultrasound-guided aspiration of Liver abscess ??
Indications for USG guided aspiration of liver abscess
1. Large abscess more than 6cms
2. Left lobe abscess
3.Caudate lobe abscess
4. Abscess which is not responding to drugs
8) INFECTIOUS DISEASE (Mucormycosis)
http://manikaraovinay.blogspot.com/2021/05/50male-came-in-altered-sensorium.html
1) QUESTION: What is the evolution of the
symptomatology in this patient in terms of an event timeline and where is the anatomical localization for the problem and what is the primary aetiology of the patient's problem?
1. 3 years ago diagnosed with hypertension
2. 21 days ago he received vaccination at local PHC which was followed by fever associated with chills and rigors, high grade fever.
3. 18 days ago he complained of similar events and went to the the local hospital, it was not subsided upon taking medication.
4. 11 days ago he complained of Generalized weakness and facial puffiness and periorbital oedema. Patient was in a drowsy state
5. 4 days ago-
a. patient presented to casualty in altered state with facial puffiness and periorbital oedema and weakness of right upper limb and lower limb
b. towards the evening patient periorbital oedema progressed
c. serous discharge from the left eye that was blood tinged
d. was diagnosed with diabetes mellitus
6. patient was referred to a government general hospital
7. patient died 2 days ago
Patient wasn't aware of his diabetic condition until then. He was also suffering from diabetic acidosis.This resulted in poorly controlled blood sugar levels. The patient was diagnosed with acute rhinocerebral mucormycosis. Rhino cerebral mucormycosis is the most common form of this fungal disease that occurs in people with uncontrolled diabetes.The fungus enters the sinuses from the environment and then the brain.
The patient was also diagnosed with acute infarct in the left frontal and temporal lobe. Mucormycosis is associated with the occurrence of CVA
2) QUESTION: What is the efficacy of drugs used along with other non-pharmacological treatment modalities and how would you approach this patient as a treating physician?
The proposed management of the patient was –
1. inj. Liposomal amphotericin B according to creatinine clearance
2. 200mg Iitraconazole was given as it was the only available drug which was adjusted to his creatinine clearance
Management of diabetic ketoacidosis –
a) Fluid replacement- The fluids will replace those lost through excessive urination, as well as help dilute the excess sugar in blood.
(b) Electrolyte replacement-The absence of insulin can lower the level of several electrolytes in blood. Patient will receive electrolytes through a vein to help keep the heart, muscles and nerve cells functioning normally.
(c) Insulin therapy- Insulin reverses the processes that cause diabetic ketoacidosis. In addition to fluids and electrolytes, patient will receive insulin therapy
Granulocyte stimulating factors may also be used in the treatment of mucormycosis.
Hyperbaric oxygen can also be used as an adjunctive therapy.
3) QUESTION: What are the postulated reasons for a sudden apparent rise in the incidence of mucormycosis in India at this point of time?
I think it is because of the use steroids in an uncontrolled manner.
COVID 19 is not the first disease where steroids are used as one of the main stay of treatment (in severe cases) but what has gone wrong in the recent time is even the lay man who got infected with Corona started using steroids right from the day 1 with no monitoring by a specialised physician.And they are not following any specific course of treatment.As many of them are also diabetic patients the are getting succumbed to mucormycosis.And it is not ending with mucormycosis but various other fungii are emerging to cause an epidemic.
And another reason for rise in mucormycosis cases may be the usage of tap water in oxygen concentrators.As most of the patients are being diagnosed of Covid in late stages in the second wave many of them Are requiring oxygen concentrators for supplemental oxygenation.And due to Lack of the people are using tap water instead of distilled water which serves as reservoir for the growth of mucormycosis.So this may be one of the reason for rise in mucormycosis cases.
9)INFECTIOUS DISEASES
http://medicinedepartment.blogspot.com/2021/05/covid-case-report-logs-from-may-2021.html?m=1
1) Sort out these detailed patient case report logs into a single web page as a master chart
2) In the master chart classify the patient case report logs into mild, moderate severe and
3) indicate for each patient, the day of covid when their severity changed from moderate to severe or vice versa recognized primarily through increasing or decreasing oxygen requirements
4) Indicate the sequence of specific terminal events for those who died with severe covid (for example, altered sensorium, hypotension etc).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Comments
Post a Comment