65 year old male patient with CKD
65 year old male patient with CKD
"This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent. Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs. This E log book also reflects my patient-centered online learning portfolio and your valuable inputs on the comment box
Chief complaints-
65 years old male patient, agriculture labourer by occupation came to general medicine OPD on 09-06-2022,with chief complaints of
fever - since 3 days
Urine retention since 2 days
Abdominal distension since 2 days
History of presenting illness-
>patient is apparently asymptomatic 3 days back.
Then he developed fever
>insidious in onset
> gradually progressive
>No diurnal variations
>Relieved on medication
> Associated with chills, rigors
>Has generalised body pains
>He developed urinary retention since 2 days.
>He developed abdominal distension since 2 days.
Not associated with pain
Past history-
He is a known case of hypertension since 4 years.
Not a known case of diabetes mellitus, tuberculosis,asthma and epilepsy.
6 months back patient had complaint of bipedal edema investigations were done ct scan showed left multiple renal calculi.
1 month back he developed fever,on and off low grade type,tightness in abdomen,facial puffiness,shortness of breath,pedal edema for which he was treated conservatively.
Surgical history-
No significant surgical history
Personal history-
.Diet-mixed
.Appetite - normal
.Sleep - adequate
.Bowel - regular
.Bladder-urinary retention since 2 days
.Allergies- none
.Alcohol- occasionally(one quarter a month)
Family history-
=>No similar complaints were present in the family members.
=>No H/O DM,HTN.
General examination-
=>Patient is conscious, coherent, co operative and well oriented to time, place, and person.
moderately build and moderately nourished.
.Temperature-99F
.Pulse rate-80 beats per minute
.Respiratory rate-17 cycles per mimute
.BP-120/80mm of Hg
.GRBS-108 mg/dl
.SpO2-95% at room air
.Pallor- present
.Icterus-absent
.cyanosis- absent
.Clubbing- absent
.Lymphadenopathy- absent
.Edema- present( gradually progressive,pitting type,bilateral,grade-3 , below knee present upto ankle region from below)
>Not relieved on rest





Systemic examination
cardio vascular examination
=> No visible pulsations, scars, engorged veins. No rise in jvp
=>Apex beat is felt at left 5th intercostal space medial to mid clavicular line.
=>S1 S2 heard . No murmurs.
- Respiratory system
=> Shape of chest is elliptical, biIlaterally symmetrical.
=> Trachea is central. Expansion of chest is symmetrical
=>Bilateral Airway entry - positive
CNS:
no sensory or motor abnormalities seen, cranial nerves:normal, higher mental functions: normal, No meningeal signs , No cerebral signs.
Local examination:
Abdomen
Patient was examined in supine position in a well lit room , with consent taken .
Inspection:
Shape of abdomen: distended
Umbilicus: inverted , central.
Movements of abdominal wall ,moves with respiration.
No visible pulsations , venous engorgement, sinuses.
Skin appears to be normal.
Palpation:
Inspectory findings confirmed,
No local raise of temperature,
Tenderness -mild tenderness in suprapubic region
Fluid thrill: not appreciated clearly
Bimanual palpation of kidney: non ballotable.
No organomegaly.
Percussion:
Normal resonant notes present over the abdomen
Auscultation:
Normal bowel sounds were heard, no bruit present



Provisional Diagnosis:
Ascites with Chronic kidney disease on maintainance hemodialysis.
Investigations:--
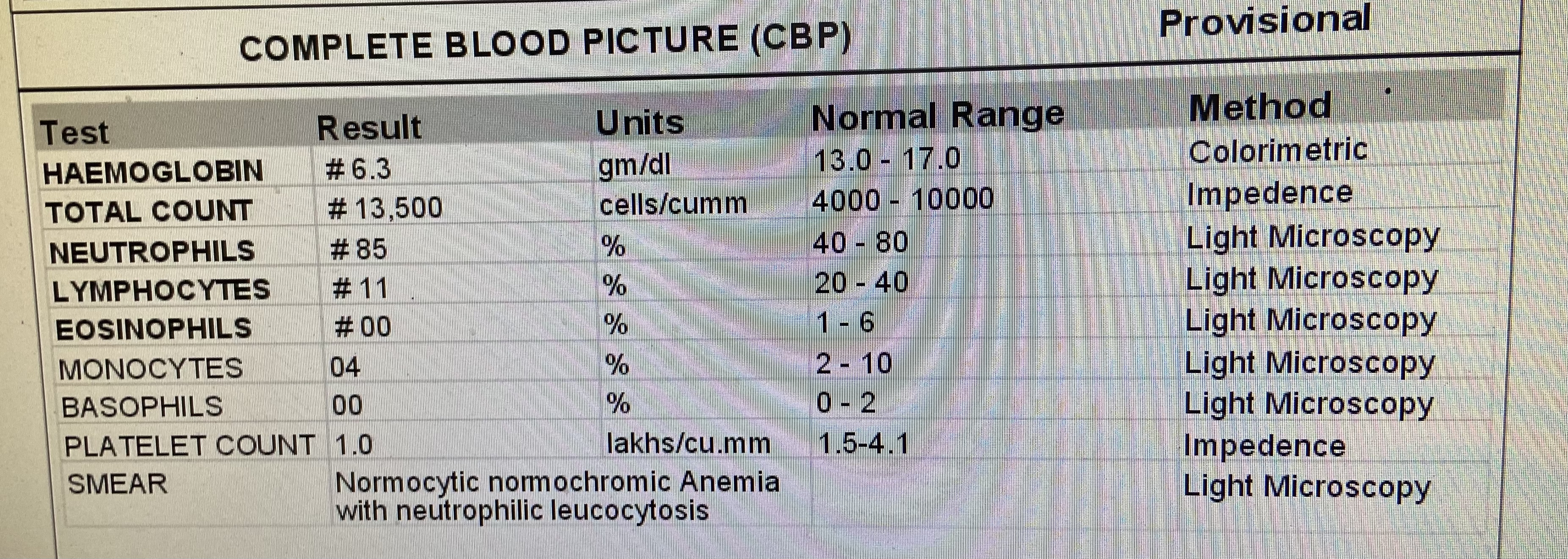
Hemogram-
On 29-05-22


RFT ON 31-05-22

LFT:-

SAAG:-

Random blood sugar-




USG report:
On 10-06-22
1)Bilateral grade -3 Renal pelvis dilation (RPD)
2) large multiple renal calculi in left kidney
3) moderate to gross ascites

Hemogram-
On 11-06-22
RFT-
On 11-06-22

Serum electrolytes-
On 11-06-22

LFT-
On 11-06-22

Treatment:
Injection. Piptaz 2.25grs,iv,/bd
Injection. Metronidazole 0.5%gm/100ml
Inj. Lasix 40 mg/i.v/stat
Tab.nodosis 500mg/po/bd
Tab. Orofer xj /po/od
Tab.shelcal 500 mg/po/od
Tab. Pan 40mg /po/ od
Tab. Nicardia 20 mg/po/bd
INJ. Iron sucrose 1 Amp /iv/od
INJ.erythropoietin 4000 U/S.C /weekly once.





Comments
Post a Comment