37 F pain in left lower limb since 2 months
This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent. Here we discuss our individual patient's problems through series of inputs from global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs. This E log book also reflects my patient-centred online learning portfolio and your valuable inputs on the comment box is welcome."I've been given this case to solve in an attempt to understand the topic of "patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with a diagnosis and treatment plan.
Complaints:
37 years female came with chief complaints of
Pain of the left lower limb since 2 months
History of presenting illness:
Patient was apparently
asymptomatic 2years back, then
develored B/L joint pains (knee), Insidious in onset, gradually progressive
No aggrerating factors and relieved on medication.
History of distal muscle weakness , difficulty in mixing food, buttonning and unbuttoning of shirt.
H/O Proximal muscle weakness, difficulty in getting from squatting position.
(diagnosed as dermatomyositis)
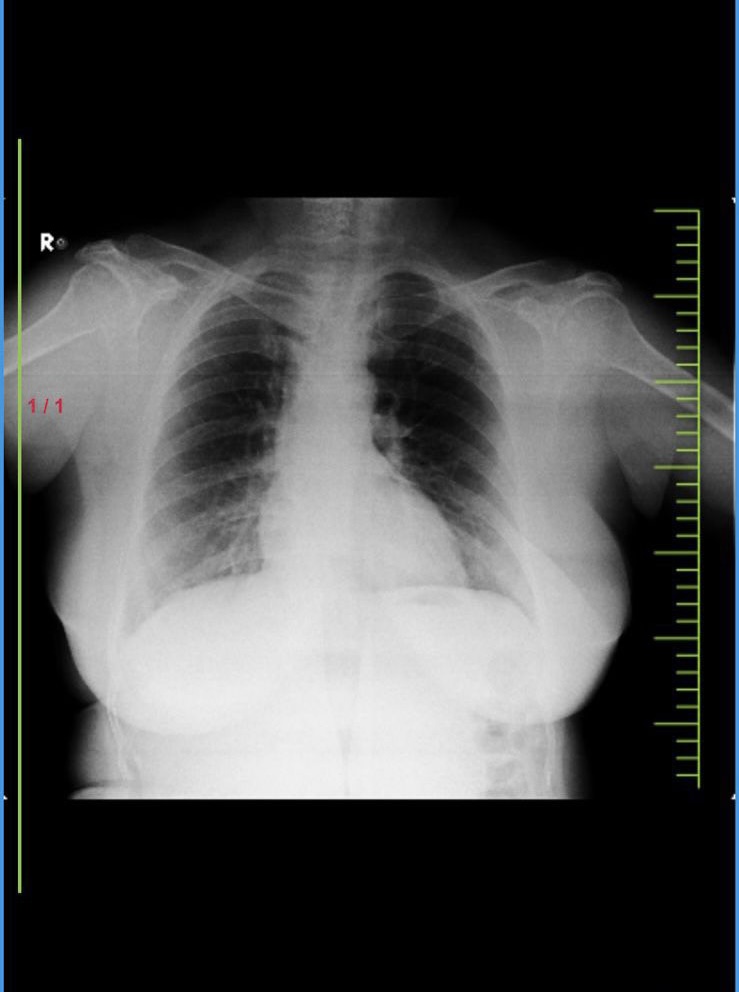
followed by 1 year back, cough with sputum, yellowish, non-foulsmelling non-blood tinged, moderate in amount, diagnosed as Pulmonary
Nocardiosis(cotrimoxazole)
Presently using:
T.Wysolone 20mg
T.Azathioprine 100mg
T.Naproxen 250mg
Now, since 2 months,
c/o Pain of the left lower limb., insidious in
Onset, gradually progressive, aggrevated by standing and walking, Not relieved with Medication(more since past 7 days),dragging type,
radiating down the leg upto ankle
C/o difficulty in getting up from sitting position since 7 days
C/o tingling and numbness of both upper and lower limbs since 7 days
polydypsia present,No polyuria, Polyphagia, Nocturia .
c/o Pedal edema since today afternoon, pitting type upto ankle
No c/o Fever, vomitings, decreased urine output, burning micturition,Chestpain,Palpitations
H/o diarrhea associated with pain abdomen 5 days back,watery stools 5-6 episodes per day,foul smelling,non blood stained
PAST HISTORY:
N/k/c/o HTN,DM,Thyroid disorders,Epilepsy
PERSONAL HISTORY:
Diet-mixed
Appetite-normal
Bowel and bladder-regular
Addictions-None
DAILY ROUTINE
She daily wakes at 5 AM and takes bath and fresh up drinks tea at 7am and then she takes her breakfast (idly/dosa) at 8am and takes her lunch at 1 pm which consisting of a vegetable curry and rice and after she chit chat with her neighbors and lie down for some time and after that she watch TV and then eats her dinner at 8pm and goes to sleep at 9pm.
FAMILY HISTORY:
Insignificant
GENERAL EXAMINATION:
Patient is conscious coherent and cooperative
No pallor ,icterus , clubbing,cyanosis,lymphadenopathy ,pedal edema
Vitals :
BP- 120/70mmhg
PR -70bpm
RR-18cpm
Spo2 99% at room air
Temperature -98.2F
SYSTEMIC EXAMINATION:
CVS: s1,s2 heard ,no Murmurs,jvp not raised
RS: BAE,no added sounds ,NVBS
P/A: soft, non tender,bowel sounds can be heard
CLINICAL IMAGES:






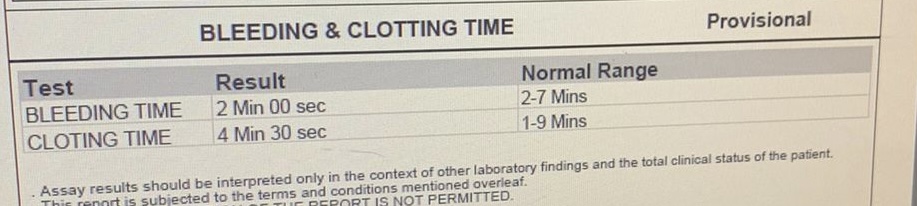
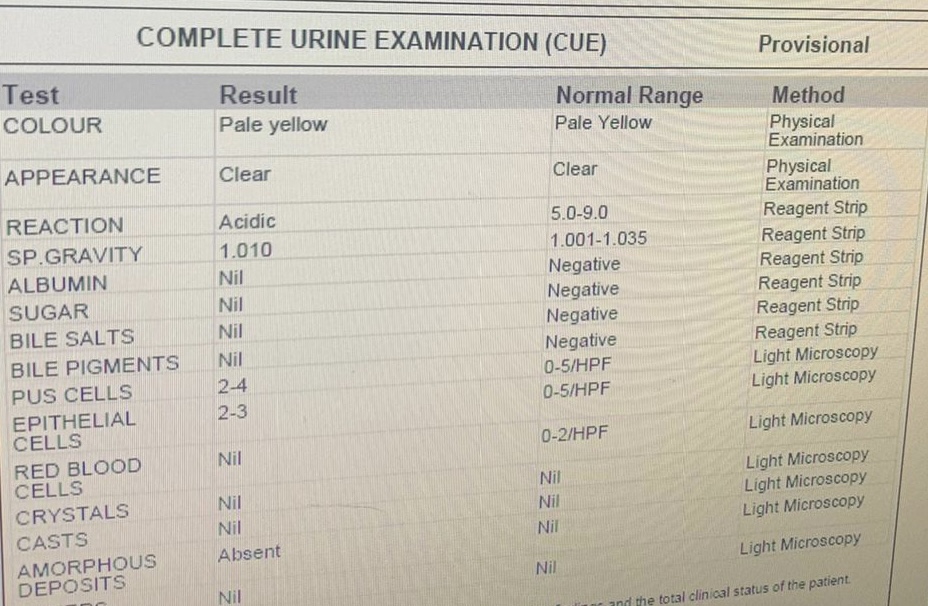
INVESTIGATIONS:
12/05/23
















MRI:




ORTHOPEDIC REFERRAL:




Diagnosis:
Dermatomyositis with pulmonary nocardiosis(resolved) with anaemia(normocytic normochromic) with Bilateral Avascular necrosis of femoral head
-Ficet and Artel stage 2 on right side,stage 3 on left side
Treatment:
T.Ultracet 1/2 tab PO QID
T.Wysolone 15mg PO OD
T.Azathioprine 100mg PO OD
SUMMARY:
Final Diagnosis:
Dermatomyositis with pulmonary nocardiosis(resolved) with anaemia(normocytic normochromic) with Bilateral Avascular necrosis of femoral head
-Ficet and Artel stage 2 on right side,stage 3 on left side
Pain of the left lower limb since 2 months
History of presenting illness:
Patient was apparently
asymptomatic 2years back, then
develored B/L joint pains (knee), Insidious in onset, gradually progressive
No aggrerating factors and relieved on medication.
History of distal muscle weakness , difficulty in mixing food, buttonning and unbuttoning of shirt.
H/O Proximal muscle weakness, difficulty in getting from squatting position.
(diagnosed as dermatomyositis)
followed by 1 year back, cough with sputum, yellowish, non-foulsmelling non-blood tinged, moderate in amount, diagnosed as Pulmonary
Nocardiosis(cotrimoxazole)
Presently using:
T.Wysolone 20mg
T.Azathioprine 100mg
T.Naproxen 250mg
Now, since 2 months,
c/o Pain of the left lower limb., insidious in
Onset, gradually progressive, aggrevated by standing and walking, Not relieved with Medication(more since past 7 days),dragging type,
radiating down the leg upto ankle
C/o difficulty in getting up from sitting position since 7 days
C/o tingling and numbness of both upper and lower limbs since 7 days
polydypsia present,No polyuria, Polyphagia, Nocturia .
c/o Pedal edema since today afternoon, pitting type upto ankle
No c/o Fever, vomitings, decreased urine output, burning micturition,Chestpain,Palpitations
H/o diarrhea associated with pain abdomen 5 days back,watery stools 5-6 episodes per day,foul smelling,non blood stained
PAST HISTORY:
N/k/c/o HTN,DM,Thyroid disorders,Epilepsy
PERSONAL HISTORY:
Diet-mixed
Appetite-normal
Bowel and bladder-regular
Addictions-None
DAILY ROUTINE
She daily wakes at 5 AM and takes bath and fresh up drinks tea at 7am and then she takes her breakfast (idly/dosa) at 8am and takes her lunch at 1 pm which consisting of a vegetable curry and rice and after she chit chat with her neighbors and lie down for some time and after that she watch TV and then eats her dinner at 8pm and goes to sleep at 9pm.
FAMILY HISTORY:
Insignificant
GENERAL EXAMINATION:
Patient is conscious coherent and cooperative
No pallor ,icterus , clubbing,cyanosis,lymphadenopathy ,pedal edema
Vitals :
BP- 120/70mmhg
PR -70bpm
RR-18cpm
Spo2 99% at room air
Temperature -98.2F
SYSTEMIC EXAMINATION:
CVS: s1,s2 heard ,no Murmurs,jvp not raised
RS: BAE,no added sounds ,NVBS
P/A: soft, non tender,bowel sounds can be heard
Course in the hospital:
Patient got admitted for c/o pain of the left lower limb since 2 months and was investigated further and ortho opinion was taken on 13/5/23 and was adviced MRI pelvis with both hips.
MRI was done on 17/5/23
Impression:
Bilateral Avascular necrosis of femoral head
-Ficet and Artel stage 2 on right side,stage 3 on left side
-Mitchell type A on right,type C on left.
Mild left hip joint effusion
Ortho review referral was done on 17/5/23 qnd was adviced Left hip core decompression first and Right hip conservative trial and the same was explained to patient and patient attenders.
Patient wants some time to get prepared for the surgical intervention and wants to get discharged.patient said that she will come next week and get admitted.
Patient vitals are stable at time of discharge.
Treatment:
T.Ultracet 1/2 tab PO QID
T.Wysolone 15mg PO OD
T.Azathioprine 100mg PO OD
Advice:
Tab.Wysolone 15mg this week ---10mg next week ----5mg following week .
Tab.Azathioprine 100mg po/od.
As advised by orthopaedic team-
Tab.osteofos 70mg po/ 1tab / week for 2months.
Tab.shelcal 500mg po/bd ,After 2months po/od.

Comments
Post a Comment